


 Sign Out
Sign Out



Fluticasone Furoate: Fluticasone furoate is a synthetic trifluorinated corticosteroid with potent, local, anti-inflammatory activity. The precise mechanism through which fluticasone furoate affects COPD and asthma symptoms is not known. Inflammation is an important component in the pathogenesis of COPD and asthma. Corticosteroids have been shown to have a wide range of actions on multiple cell types (e.g., mast cells, eosinophils, neutrophils, basophils, macrophages, lymphocytes) and mediators (e.g., histamine, eicosanoids, leukotrienes, cytokines) involved in inflammation. Specific effects of fluticasone furoate demonstrated in in vitro and in vivo models included activation of the glucocorticoid response element, inhibition of pro-inflammatory transcription factors such as NFkB resulting in inhibition of pro-inflammatory cytokines, and inhibition of antigen-induced lung eosinophilia in sensitized rats. These anti-inflammatory actions of corticosteroids may contribute to their efficacy.
Fluticasone furoate has been shown in vitro to exhibit a binding affinity for the human glucocorticoid receptor that is approximately 29.9 times that of dexamethasone and 1.7 times that of fluticasone propionate. Although fluticasone furoate is structurally related to fluticasone propionate, they are distinct chemical entities and do not share common metabolites. In vitro studies have shown that translocation of the glucocorticoid receptor into the cell nucleus (essential for anti-inflammatory activity) is both more rapid and more prolonged with fluticasone furoate compared with fluticasone propionate. Nuclear localization of the glucocorticoid receptor was observed at 30 hours post-exposure with fluticasone furoate but not with fluticasone propionate. The clinical relevance of these findings is unknown.
Umeclidinium: Umeclidinium is a long-acting muscarinic antagonist (LAMA) [also referred to as a long-acting anticholinergic (LAAC)]. It is a quinuclidine derivative that is a muscarinic receptor antagonist with activity across multiple muscarinic cholinergic receptor subtypes. Umeclidinium exerts its 24-hour bronchodilatory activity by competitively inhibiting the binding of acetylcholine with muscarinic acetylcholine receptors on airway smooth muscle. It demonstrates slow reversibility at the human M3 muscarinic receptor subtype in vitro and a long duration of action in vivo when administered directly to the lungs in pre-clinical models.
Vilanterol: Vilanterol is a selective high-affinity long acting beta2-agonist (LABA), with bronchodilatory effects maintained for 24-hours. The pharmacologic effects of beta2-agonists, including vilanterol, are at least in part attributable to stimulation of intracellular adenylate cyclase, the enzyme that catalyzes the conversion of adenosine triphosphate (ATP) to cyclic-3',5'-adenosine monophosphate (cyclic AMP). Increased cyclic AMP levels cause relaxation of bronchial smooth muscle and inhibition of release of mediators of immediate hypersensitivity from cells, especially from mast cells. Although beta2-receptors are the predominant adrenergic receptors in bronchial smooth muscle and beta1-receptors are the predominant receptors in the heart, there are also beta2-receptors in the human heart comprising 10% to 50% of the total beta-adrenergic receptors. The precise function of these receptors has not been established, but they raise the possibility that even highly selective beta2-agonists may have cardiac effects.
Pharmacodynamics: Time to Onset of Action: In a study of TRELEGY ELLIPTA (fluticasone furoate/umeclidinium/vilanterol) 100/62.5/25 mcg once daily, serial spirometry measures were obtained from a subgroup of 203 subjects with COPD. On Day 1, 49% of subjects achieved an increase of ≥100 mL over baseline FEV1 at 15 minutes (time of first serial spirometry sample). Median time to onset of action was 26 minutes.
HPA Axis Effects: Effects on HPA-axis function are known to occur with systemic administration of corticosteroids and this systemic side effect has also been reported with inhaled and intranasal corticosteroid use.
Based on both clinical pharmacology and clinical data, inhaled fluticasone furoate at repeat doses up to 400 mcg was not consistently associated with statistically significant decreases in serum or urinary cortisol in healthy subjects. At higher doses, above the therapeutic range, corticosteroid class-related decreases in serum and urine cortisol levels were observed. In line with the increased fluticasone furoate systemic exposure, serum cortisol was reduced by approximately a third in subjects with moderate hepatic impairment after fluticasone furoate/vilanterol 200/25 mcg administration and a similar effect would be anticipated in subjects with severe hepatic impairment at this dose.
Class-Related Beta2-Adrenoceptor Systemic Effects: Class-related systemic effects that are known to occur with systemic administration of beta-agonists include hypokalaemia, hyperglycaemia, and increases in blood pressure, heart rate and the QTc interval. Following inhaled administration these effects are limited by local topical administration in the lung, low clinical doses and first pass metabolism of the swallowed portion of the dose and also tended to diminish on repeat dosing.
The clinical pharmacology data indicate that vilanterol 25 mcg is not associated with clinically significant class-related beta2-adrenoceptor systemic effects. Vilanterol, administered either alone or in combination with fluticasone furoate at doses up to 50 mcg was not associated with clinically relevant or statistically significant effects on blood potassium or blood glucose. Vilanterol 100 mcg was associated with a small decrease in blood potassium (approximately ≤0.1 mmol/L) and a small increase in blood glucose (approximately <1 mmol/L). Vilanterol at doses up to 100 mcg was not consistently associated with clinically relevant or statistically significant effects on blood pressure. Where PD effects were seen, there was no evidence of an increased effect with repeat dosing while some effects showed signs of diminishing.
Cardiovascular Effects: Fluticasone Furoate/Umeclidinium/Vilanterol: The effect of fluticasone furoate/umeclidinium/vilanterol on the QT interval has not been evaluated in a thorough QT (TQT) study.
No clinically relevant effects on the QTc interval were observed on review of centrally read ECGs from 766 subjects with asthma exposed to TRELEGY ELLIPTA for up to 24 weeks, or in a subset of 178 subjects exposed for up to 52 weeks.
No clinically relevant effects on the QTc interval were observed on review of centrally read ECGs from 911 subjects with COPD exposed to fluticasone furoate/umeclidinium/vilanterol for up to 24 weeks, or in a subset of 210 subjects exposed for up to 52 weeks.
The effect of TRELEGY ELLIPTA on cardiac rhythm in subjects diagnosed with COPD was assessed using 24-hour Holter monitoring in a subset of subjects in a 24-week active comparator study: 212 subjects receiving TRELEGY ELLIPTA for 24 weeks were assessed. No clinically meaningful effects on cardiac rhythm were observed following 24 weeks of treatment.
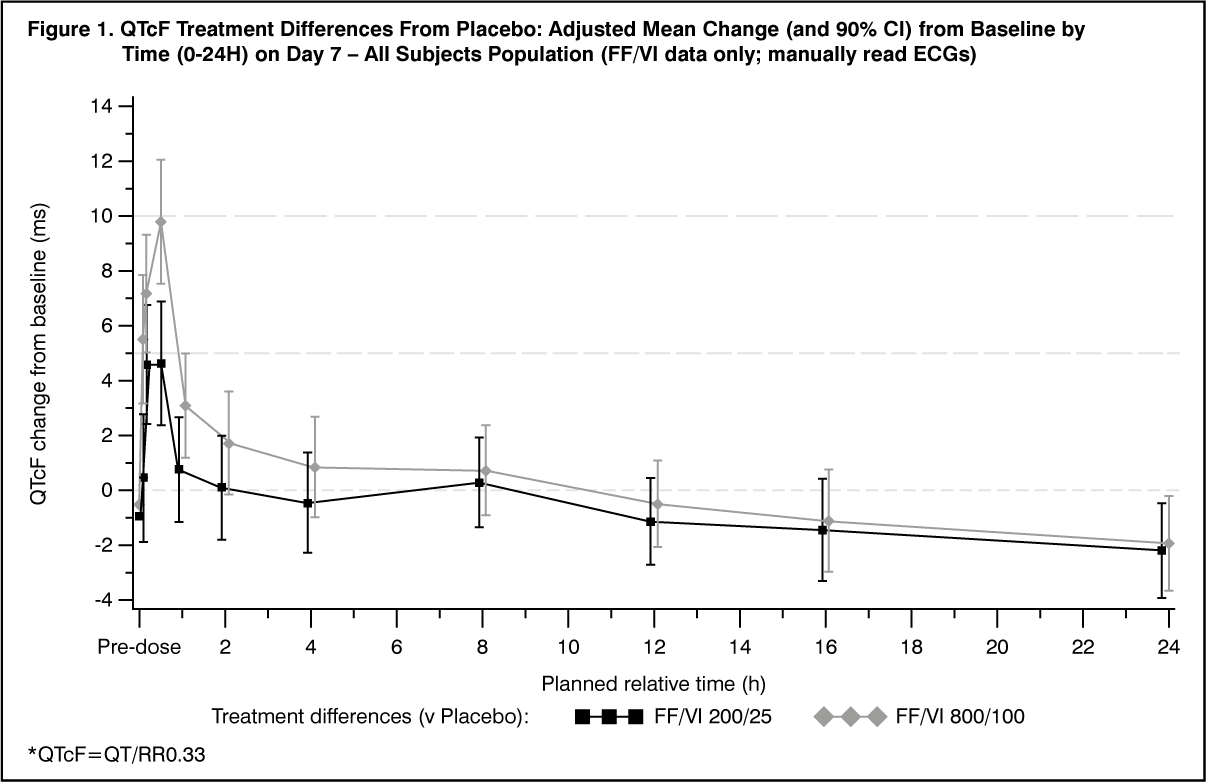
Fluticasone Furoate/Vilanterol: The effect of fluticasone furoate/vilanterol on ECG parameters was investigated in 85 healthy subjects in a double-blind, randomised, placebo- and active-controlled, 4-way crossover study. Fluticasone furoate/vilanterol 200/25 mcg and fluticasone furoate/vilanterol 800/100 mcg were administered once daily for 7 days. The fluticasone furoate/vilanterol dose represented up to 4 times the recommended dose of vilanterol in fluticasone furoate/vilanterol, and a 10 or 12-fold higher vilanterol systemic exposure than seen in patients with asthma and COPD, respectively.
Increases in the QTcF interval were observed that were maximal at 30 min post-dosing. At the 30 min time point, the placebo-adjusted mean changes from baseline in the QTcF interval (ms) were 4.5 (90% CI: 2.1, 6.9) in the fluticasone furoate/vilanterol 200/25 mcg treatment arm and 9.6 (90% CI: 7.2, 12.0) in the fluticasone furoate/vilanterol 800/100 mcg treatment arm. (See Figure 1.)
 Click on icon to see table/diagram/image
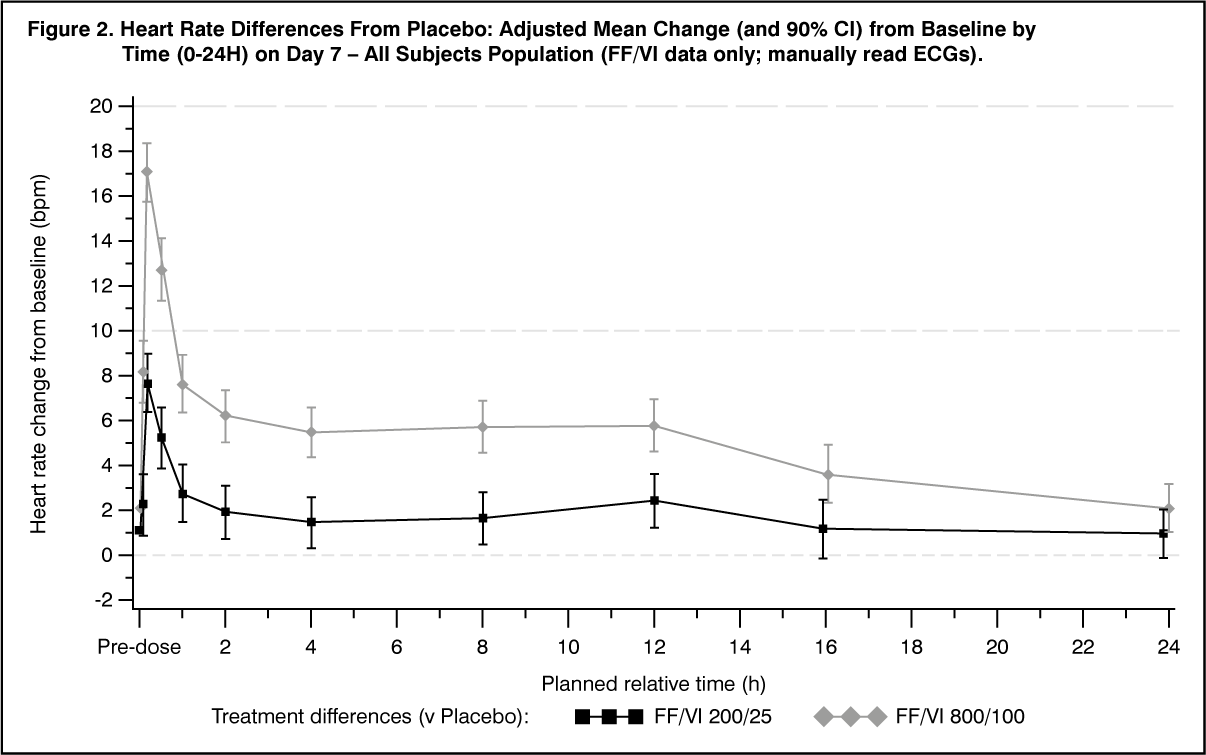
Click on icon to see table/diagram/imageIncreases in heart rate were observed that were maximal at 10 min. At the 10 min time point, the placebo-adjusted mean change from baseline in heart rate (bpm) was 7.6 (90% CI: 6.3, 8.9) in the fluticasone furoate/vilanterol 200/25 mcg treatment arm and 17.0 (90% CI: 15.7, 18.3) in the fluticasone furoate/vilanterol 800/100 mcg treatment arm. (See Figure 2.)
 Click on icon to see table/diagram/image
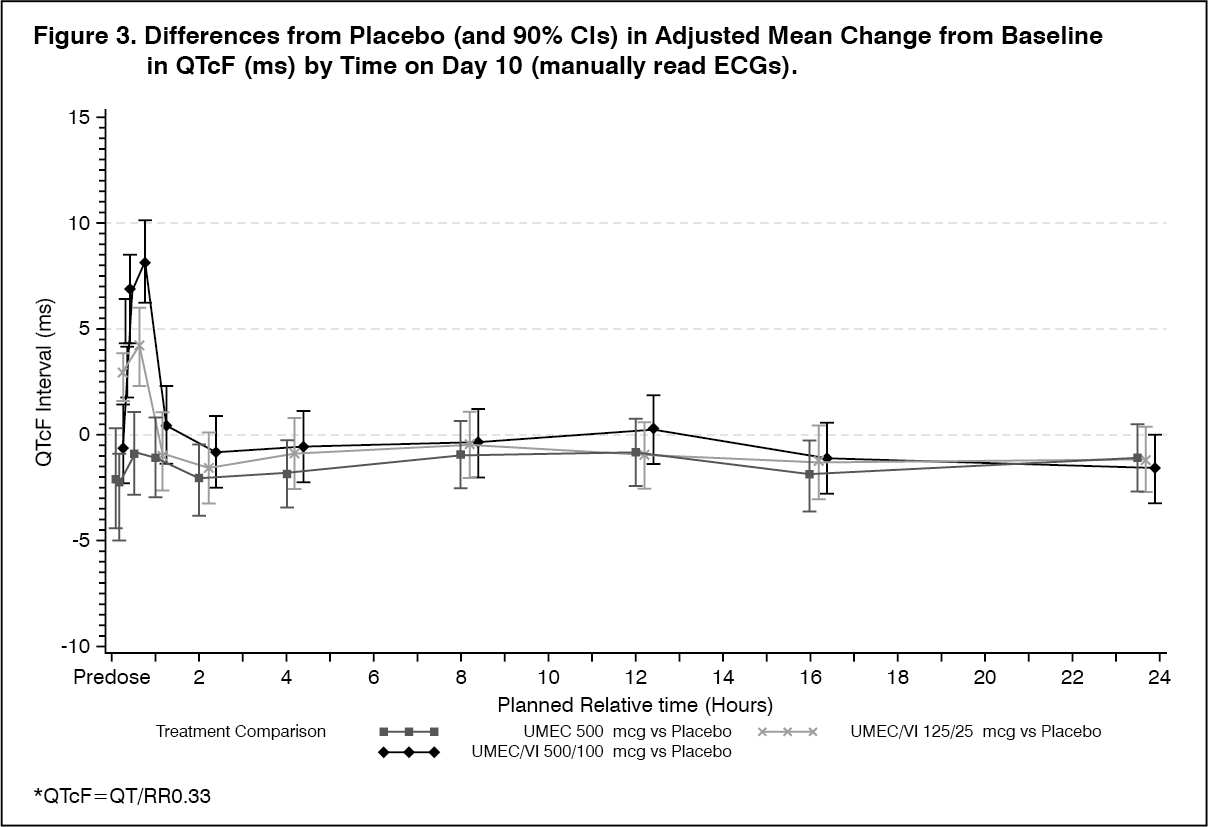
Click on icon to see table/diagram/imageUmeclidinium/Vilanterol: The effect of umeclidinium/vilanterol on ECG parameters was investigated in 103 healthy subjects in a double-blind, randomized, placebo- and active-controlled, incomplete block, crossover study. Umeclidinium alone at a dose of 500 mcg and umeclidinium/vilanterol at supratherapeutic doses of 125/25 mcg (2X/1X therapeutic dose) and 500/100 mcg (8X/4X therapeutic dose) were studied once daily for 10 days.
Increases in the QTcF interval were observed that were maximal at 10 min (umeclidinium/vilanterol 125/25 mcg) and 30 min (umeclidinium/vilanterol 500/100 mcg) post-dosing. The maximal placebo-adjusted mean change in the QTcF interval was 4.3 ms (90% CI: 2.2, 6.4) at 10 min for the 125/25 mcg dose and 8.2 ms (90% CI: 6.2, 10.2) at 30 min for the 500/100 mcg dose.
Umeclidinium 500 mcg alone was not associated with QTc prolongation. (See Figure 3.)
 Click on icon to see table/diagram/image
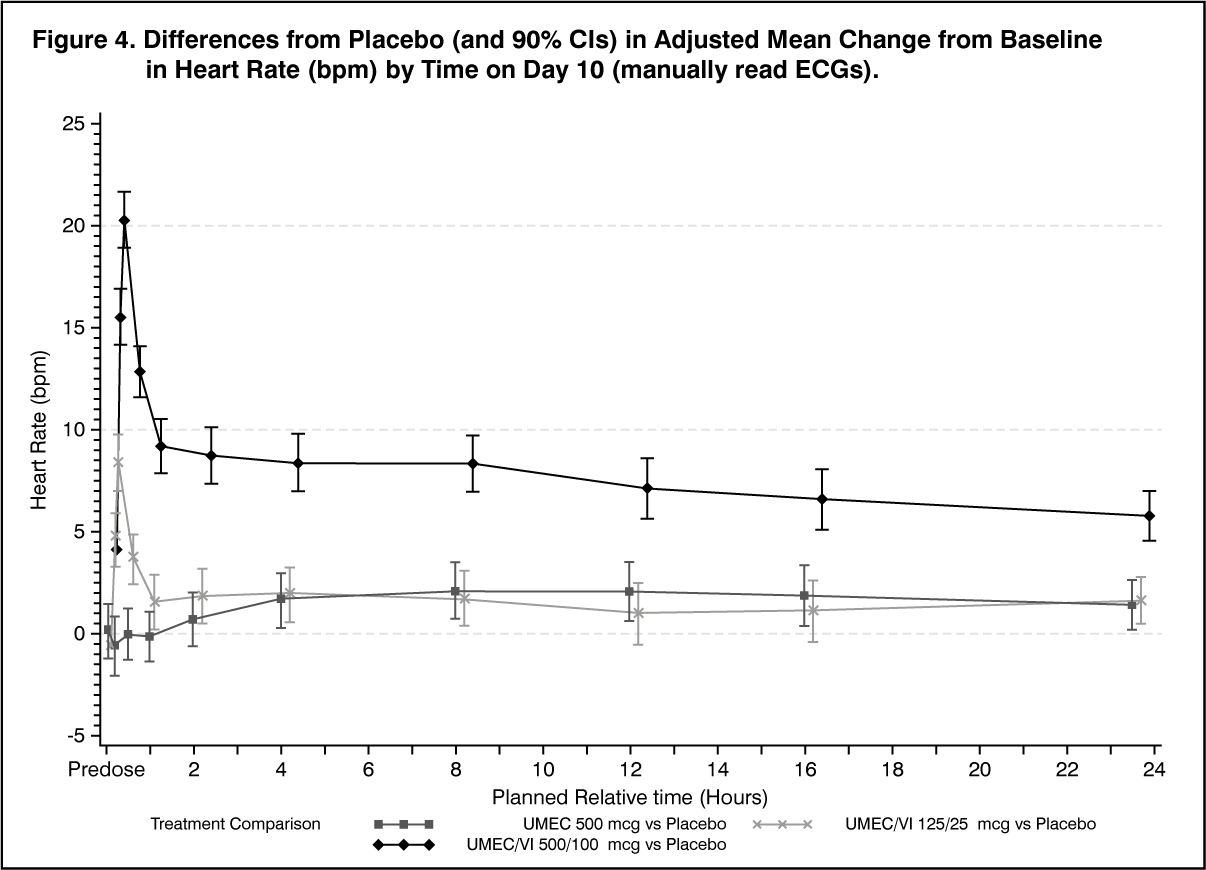
Click on icon to see table/diagram/imageA dose-dependent increase in heart rate was also observed with the administration of umeclidinium/vilanterol. The maximum mean difference in heart rate from placebo after baseline-correction was 8.4 (90% CI: 7.0, 9.8) beats/min and 20.3 (90% CI: 18.9, 21.7) beats/min seen 10 minutes after dosing for umeclidinium/vilanterol 125/25 mcg and umeclidinium/vilanterol 500/100 mcg, respectively.
Umeclidinium 500 mcg was associated with small positive mean differences from placebo in heart rate from 4 to 24 h, inclusive, with a maximum mean difference of 2.1 bpm (90% CI: 0.7, 3.5) at 8 h. (See Figure 4.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageAdditional trials: Studies 200109 and 200110 were 12-week randomized, double-blind, parallel-group studies of umeclidinium 62.5 mcg + fluticasone furoate/vilanterol 100/25 mcg once-daily compared to placebo + fluticasone furoate/vilanterol 100/25 mcg. The primary endpoint was change from baseline in trough (predose) FEV1 at Day 85 (defined as the mean of the FEV1 values obtained at 23 and 24 hours after the previous dose on Day 84).
The results showed that patients treated with umeclidinium 62.5 mcg + fluticasone furoate/vilanterol 100/25 mcg had statistically significant greater mean changes from baseline in trough FEV1 relative to placebo + fluticasone furoate/vilanterol 100/25 mcg (124 mL, 95% CI: 93-154 mL; 122 mL 95% CI: 91-152 mL).
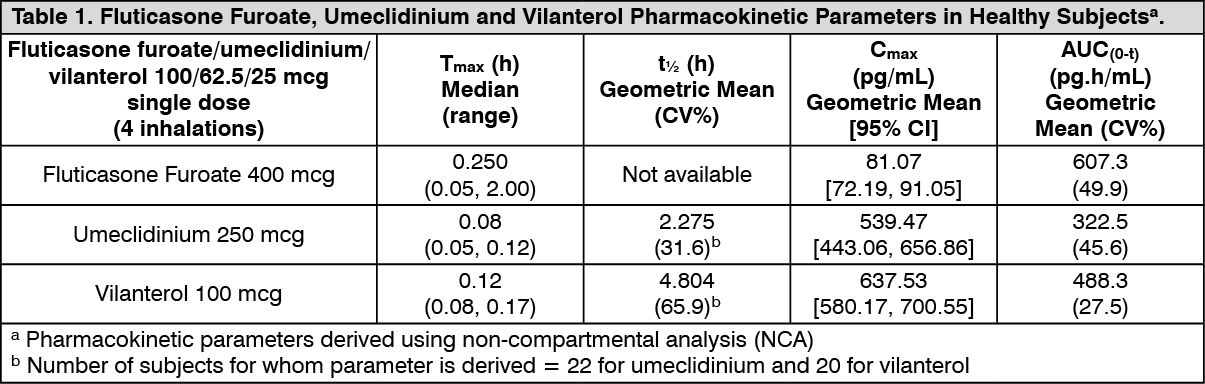
Pharmacokinetics: The systemic pharmacokinetics of the components of TRELEGY ELLIPTA 100/62.5/25 mcg was assessed in 43 healthy subjects. Four inhalations of fluticasone furoate/umeclidinium/vilanterol 100/62.5/25 mcg were administered as a single dose (see Table 1).
 Click on icon to see table/diagram/image
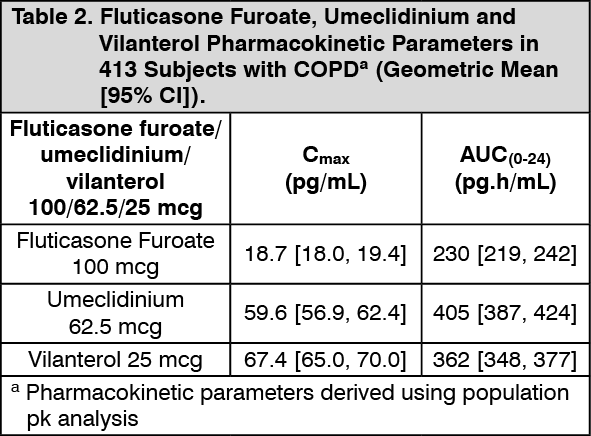
Click on icon to see table/diagram/imageCOPD: Population PK analyses for TRELEGY ELLIPTA were conducted using a combined dataset from three phase III studies in 821 COPD subjects, including 413 subjects who received TRELEGY ELLIPTA 100/62.5/25 mcg. Steady state Cmax and AUC0-24 values of fluticasone furoate, umeclidinium and vilanterol following administration of TRELEGY ELLIPTA 100/62.5/25 mcg in one inhaler are presented in Table 2. (See Table 2.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageCovariate analysis showed higher fluticasone furoate apparent clearance (42%) when comparing fluticasone furoate/vilanterol to fluticasone furoate/umeclidinium/vilanterol; however, this is not considered clinically relevant.
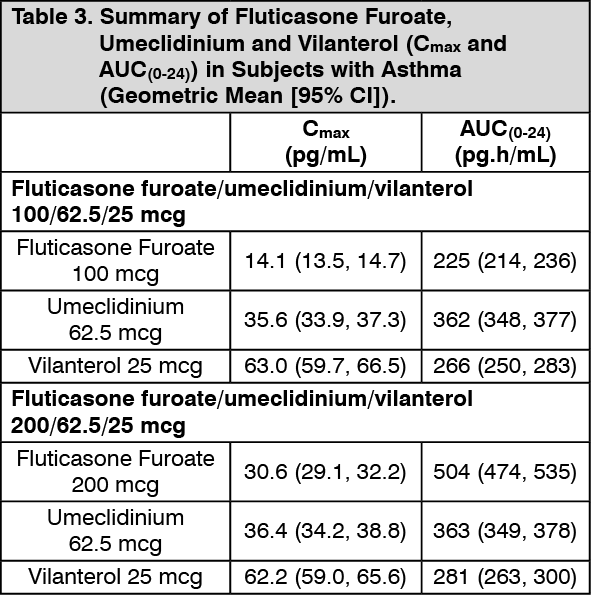
Asthma: The systemic pharmacokinetics of the components of TRELEGY ELLIPTA was assessed in subjects with asthma (1,265 subjects for fluticasone furoate; 634 subjects for umeclidinium; 1,263 subjects for vilanterol) via population PK approach. In these analyses, systemic drug levels (steady-state Cmax and AUC0-24) of fluticasone furoate and vilanterol following fluticasone furoate/umeclidinium/vilanterol (100/62.5/25 mcg and 200/62.5/25 mcg) in one inhaler (triple combination) were within the range of those observed following administration of the dual combination of fluticasone furoate/vilanterol with respect to 100 mcg and 200 mcg fluticasone furoate doses. The systemic exposure of umeclidinium 62.5 mcg following fluticasone furoate/umeclidinium/vilanterol in one inhaler was within the range of those observed following administration of umeclidinium 62.5 mcg as monotherapy.
Steady state Cmax and AUC0-24 values of fluticasone furoate, umeclidinium and vilanterol following administration of TRELEGY ELLIPTA 100/62.5/25 mcg and 200/62.5/25 mcg in one inhaler are presented in Table 3. (See Table 3.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageAbsorption: Fluticasone Furoate: Following inhaled administration of fluticasone furoate/umeclidinium/vilanterol in healthy subjects, fluticasone furoate Cmax occurred at 15 minutes. The absolute bioavailability of fluticasone furoate when administrated as fluticasone furoate/vilanterol by inhalation was on average 15.2%, primarily due to absorption of the inhaled portion of the dose delivered to the lung, with negligible contribution from oral absorption. Following repeat dosing of inhaled fluticasone furoate/vilanterol, steady state was achieved within 6 days with up to 1.6-fold accumulation.
Umeclidinium: Following inhaled administration of fluticasone furoate/umeclidinium/vilanterol in healthy subjects, umeclidinium Cmax occurred at 5 minutes. The absolute bioavailability of inhaled umeclidinium was on average 13%, with negligible contribution from oral absorption. Following repeat dosing of inhaled umeclidinium, steady state was achieved within 7 to 10 days with 1.5 to 2-fold accumulation.
Vilanterol: Following inhaled administration of fluticasone furoate/umeclidinium/vilanterol in healthy subjects, vilanterol Cmax occurred at 7 minutes. The absolute bioavailability of inhaled vilanterol when administered as fluticasone furoate/vilanterol by inhalation was on average 27%, with negligible contribution from oral absorption. Following repeat dosing of inhaled fluticasone furoate/vilanterol, steady state was achieved within 6 days with up to 1.5-fold accumulation.
Distribution: Fluticasone Furoate: Following intravenous administration to healthy subjects, the mean volume of distribution at steady state was 661 L. The binding of fluticasone furoate to human plasma proteins was high (99.6%).
Umeclidinium: Following intravenous administration to healthy subjects, the mean volume of distribution was 86 L. In vitro plasma protein binding in human plasma was on average 89%.
Vilanterol: Following intravenous administration to healthy volunteers, the mean volume of distribution at steady state was 165 L. In vitro plasma protein binding in human plasma was on average 94%.
Metabolism: Fluticasone Furoate: In vitro studies showed that fluticasone furoate is metabolised principally by CYP3A4 and is a substrate for the P-glycoprotein (P-gp) transporter. Fluticasone furoate is primarily metabolised through hydrolysis of the S-fluoromethyl carbothioate group to metabolites with significantly reduced corticosteroid activity. Systemic exposure to the metabolites is low.
Umeclidinium: In vitro studies showed that umeclidinium is metabolized principally by CYP2D6 and is a substrate for the P-gp transporter. The primary metabolic routes for umeclidinium are oxidative (hydroxylation, O-dealkylation) followed by conjugation (e.g., glucuronidation, etc.), resulting in a range of metabolites with either reduced pharmacological activity or for which the pharmacological activity has not been established. Systemic exposure to the metabolites is low.
Vilanterol: In vitro studies showed that vilanterol was metabolized principally via CYP3A4 and is a substrate for the P-gp transporter. The primary metabolic routes are O-dealkylation to a range of metabolites with significantly reduced beta1-and beta2-agonist activity. Plasma metabolic profiles following oral administration of vilanterol in a human radiolabel study were consistent with high first-pass metabolism. Systemic exposure to the metabolites is low.
Elimination: Fluticasone Furoate: Fluticasone furoate and its metabolites are eliminated primarily in the feces, accounting for approximately 101% and 90% of the orally and intravenously administered dose, respectively. Urinary excretion accounted for approximately 1% and 2% of the orally and intravenously administered doses, respectively. Following repeat-dose inhaled administration, the plasma elimination phase half-life averaged 24 hours.
Umeclidinium: Plasma clearance following intravenous administration was 151 L/hr. Following intravenous administration, approximately 58% of the administered radiolabeled dose (or 73% of the recovered radioactivity) was excreted in feces and 22% of the administered radiolabelled dose (27% of recovered radioactivity) in urine. The excretion of the drug-related material in the feces following intravenous dosing indicated secretion into the bile. Following oral administration to healthy male subjects, total radioactivity was excreted primarily in feces (92% of the administered radiolabelled dose). Less than 1% of the orally administered dose was excreted in urine, suggesting negligible absorption following oral administration. Umeclidinium plasma elimination half-life following inhaled dosing for 10 days averaged 19 hours, with 3% to 4% drug excreted unchanged in urine at steady-state.
Vilanterol: Plasma clearance of vilanterol following intravenous administration was 108 L/hr. Following oral administration of radiolabelled vilanterol, mass balance showed 70% of the radiolabel in urine and 30% in feces. Primary elimination of vilanterol was by metabolism followed by excretion of metabolites in urine and feces. Vilanterol plasma elimination half-life following inhaled dosing for 10 days averaged 11 hours.
Special Populations and Conditions: Pediatrics: The safety and efficacy of TRELEGY ELLIPTA in pediatric patients below 18 years of age have not been established.
Effects on Growth: Inhaled corticosteroids may cause a reduction in growth velocity when administered to children and adolescents. A reduction of growth velocity in children and adolescents may occur as a result of poorly controlled asthma or from use of corticosteroids, including inhaled corticosteroids. The effects of long-term treatment of children and adolescents with inhaled corticosteroids, including fluticasone furoate, on final adult height are not known.
Controlled clinical trials have shown that inhaled corticosteroids may cause a reduction in growth in children. In these trials, the mean reduction in growth velocity was approximately 1 cm/year (range: 0.3 to 1.8 cm/year) and appears to be related to dose and duration of exposure. This effect has been observed in the absence of laboratory evidence of HPA axis suppression, suggesting that growth velocity is a more sensitive indicator of systemic corticosteroid exposure in children than some commonly used tests of HPA axis function. The long-term effects of this reduction in growth velocity associated with inhaled corticosteroids, including the impact on final adult height, are unknown. The potential for "catch-up" growth following discontinuation of treatment with inhaled corticosteroids has not been adequately studied.
A randomized, double-blind, parallel-group, multicenter, 1-year, placebo-controlled trial evaluated the effect of once-daily treatment with 110 mcg of fluticasone furoate in the nasal spray formulation on growth velocity assessed by stadiometry. The subjects were 474 pre-pubescent children (girls aged 5 to 7.5 years and boys aged 5 to 8.5 years). Mean growth velocity over the 52-week treatment period was lower in the patients receiving fluticasone furoate nasal spray (5.19 cm/year) compared with placebo (5.46 cm/year). The mean reduction in growth velocity was 0.27 cm/year (95% CI: 0.06 to 0.48) (see Endocrine and Metabolism under Precautions).
Geriatrics: The effects of age on the pharmacokinetics of fluticasone furoate, umeclidinium and vilanterol were evaluated in population pharmacokinetic analyses. No clinically relevant effects requiring dose adjustment were observed for subjects with COPD or asthma.
Sex: In population pharmacokinetic analyses in subjects with COPD or asthma, no clinically relevant differences requiring dose adjustment based on gender were observed in fluticasone furoate, umeclidinium or vilanterol systemic exposure.
Ethnic origin: No clinically relevant differences requiring dose adjustment in COPD or asthma based on race were observed in fluticasone furoate, umeclidinium or vilanterol systemic exposure.
In 113 East Asian subjects with COPD (Japanese and East Asian Heritage), who received fluticasone furoate/umeclidinium/vilanterol 100/62.5/25 mcg from a single inhaler (27% subjects), fluticasone furoate and umeclidinium AUCSS estimates were on average 30% and 33%, respectively, higher compared with Caucasian subjects. However, these higher fluticasone furoate systemic exposures remain below the threshold for fluticasone furoate-induced reduction of serum and urine cortisol and are not considered clinically relevant. Also, these higher umeclidinium systemic exposures are not expected to be clinically relevant with respect to safety in these subjects.
There was no effect of race on pharmacokinetic parameter estimates of vilanterol in subjects with COPD.
In 92 East Asian subjects with asthma (Japanese, East Asian and Southeast Asian heritage) who provided fluticasone furoate/umeclidinium/vilanterol (100/62.5/25 mcg or 200/62.5/25 mcg) population pharmacokinetic data, estimates of vilanterol Cmax at steady state was approximately 3-fold higher than non-East Asian subjects.
There was no effect of race on pharmacokinetics of fluticasone furoate or umeclidinium in subjects with asthma.
Hepatic Insufficiency: Fluticasone furoate/umeclidinium/vilanterol has not been evaluated in subjects with hepatic impairment. However, studies have been conducted with fluticasone furoate/vilanterol and umeclidinium/vilanterol.
The impact of hepatic impairment on the pharmacokinetics of combination doses of fluticasone furoate/vilanterol was evaluated in patients with mild (n=9), moderate (n=9) and severe (n=8) hepatic insufficiency, stratified using the Child-Pugh classification. Subjects with mild or moderate hepatic impairment and healthy control subjects (n=9) received fluticasone furoate/vilanterol 200/25 mcg once daily for 7 days. As a precaution, subjects with severe hepatic impairment received a lower combination dose of fluticasone furoate/vilanterol 100/12.5 mcg once daily for 7 days. There was an increase in fluticasone furoate systemic exposure (up to 3-fold increase in AUC(0-24)) in subjects with mild, moderate, or severe hepatic impairment compared with healthy subjects. No clinically relevant effects on weighted mean serum cortisol were observed in subjects with mild hepatic impairment. In subjects with moderate hepatic impairment, mean serum cortisol (0 to 24 hours) was reduced by 34% compared with healthy subjects. Hepatic impairment had no effect on vilanterol systemic exposure. For patients with moderate or severe hepatic impairment the maximum dose is TRELEGY ELLIPTA 100/62.5/25 mcg (see Dosage & Administration).
The pharmacokinetics of umeclidinium and vilanterol following co-administration have been evaluated in subjects with moderate hepatic impairment (Child-Pugh score of 7-9). There was no evidence of an increase in systemic exposure to either umeclidinium or vilanterol (Cmax and AUC), and no evidence of altered protein binding between subjects with moderate hepatic impairment and healthy volunteers. Umeclidinium has not been evaluated in subjects with severe hepatic impairment.
Renal Insufficiency: Fluticasone furoate/umeclidinium/vilanterol has not been evaluated in subjects with renal impairment. However, studies have been conducted with fluticasone furoate/vilanterol and umeclidinium/vilanterol.
A clinical pharmacology study of fluticasone furoate/vilanterol showed that severe renal impairment (creatinine clearance <30mL/min) did not result in significantly greater exposure to fluticasone furoate or vilanterol compared with healthy subjects.
The pharmacokinetics of umeclidinium and vilanterol following co-administration have been evaluated in subjects with severe renal impairment (creatinine clearance <30 mL/min). Umeclidinium systemic exposure was not significantly increased (10% for AUC) and vilanterol systemic exposure (AUC(0-24)) was 56% higher in subjects with severe renal impairment compared with healthy subjects. There was no evidence of altered protein binding between subjects with severe renal impairment and healthy volunteers.